Solar Retinopathy – April, 2023

History:
A 20-year-old male presented with dark spots in both eyes. He endorsed staring at the sun for an extended period of time about 1 week prior to presentation. He denied any past medical or ocular history. He did not take any daily medications.
Exam:
His visual acuity was 20/30 in both eyes. His pupils were normally reactive without RAPD. Intraocular pressure was 15 in both eyes. Anterior segment exam was normal in both eyes. His dilated exam was significant for mild retinal pigment epithelial changes in the fovea in both eyes. The peripheral exam was normal.
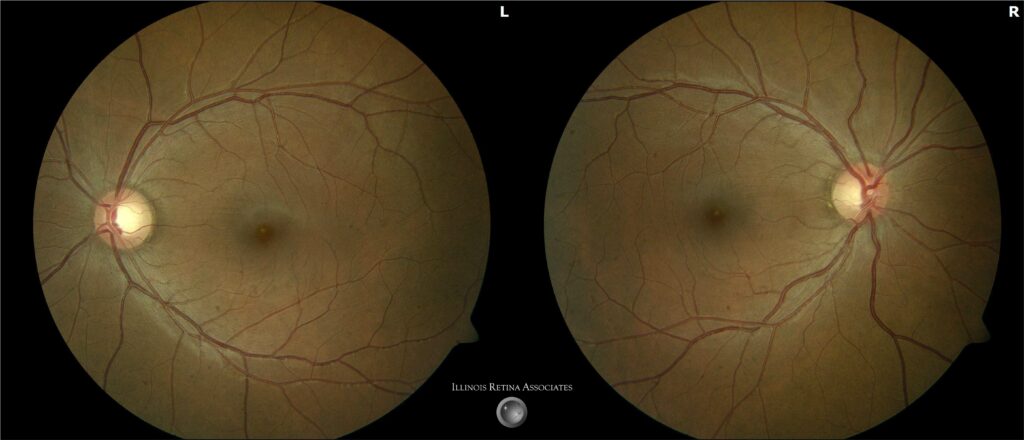
Figure 1: Fundus photography of both eyes showed subtle hypopigmentation in the fovea.
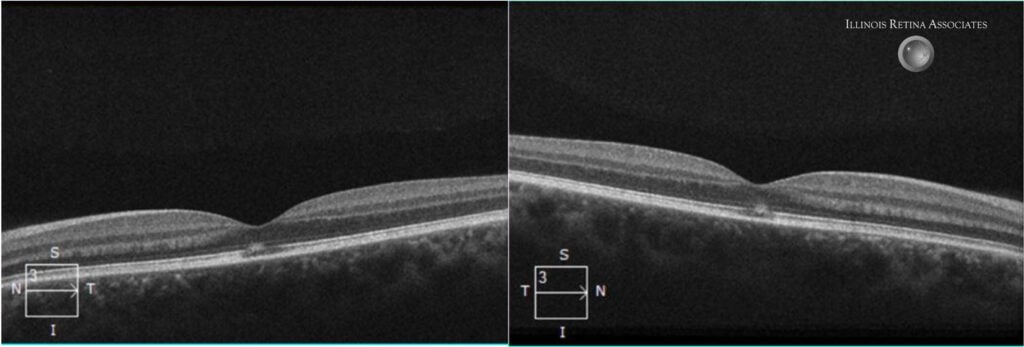
Figure 2: Optical coherence tomography of the macula showed subfoveal ellipsoid zone changes in both eyes.
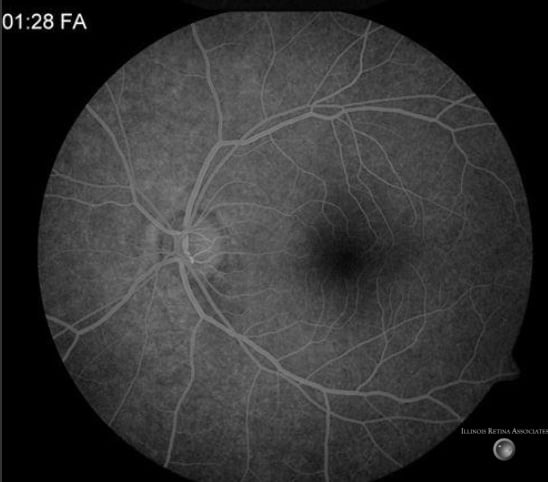
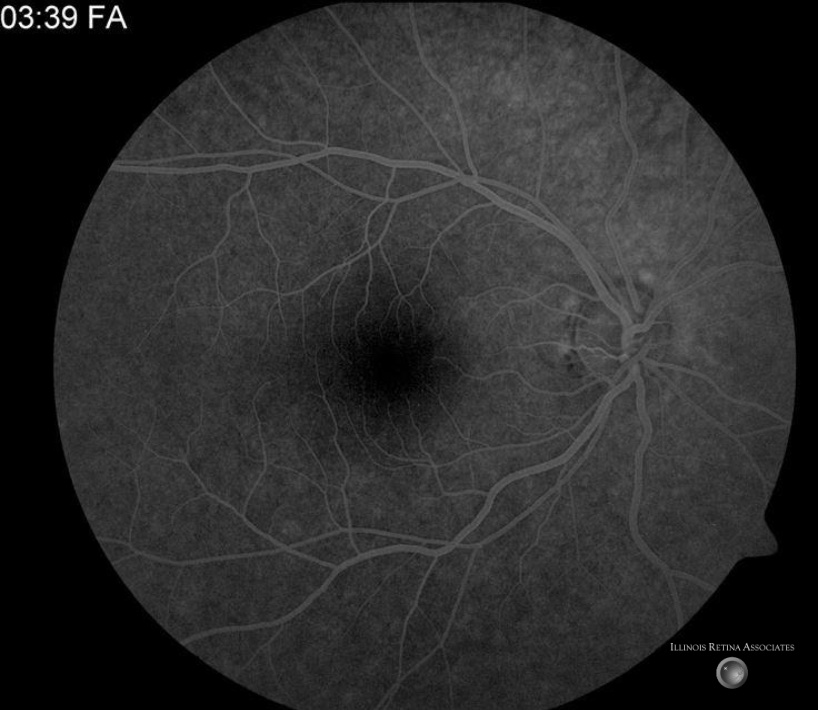
Figure 3: Fluorescein angiography showed with normal transit times without significant leakage, staining, or window defects in the posterior pol.
Differential Diagnosis:
-
Macular dystrophies (e.g. Best disease or pattern dystrophy) - Vitreomacular interface disease (e.g. vitreomacular adhesion or vitreomacular traction)
- Solar retinopathy
- Drug related maculopathy
- Cystoid macular edema
Discussion:
Solar Retinopathy
Solar retinopathy, also known as photic retinopathy, foveomacular retinitis, solar retinitis, and eclipse retinopathy, results from photochemical toxicity and leads to injury to the retinal layers, typically in the fovea. The photochemical injury to the retina leads to free radical production and subsequent damage. The main risk factor is extended exposure to high intensity light. Other risk factors include young age, clear lenses, photosensitizing medications like tetracyclines, and mental impairment such as psychiatric illness or illicit drug use.
The diagnosis of solar retinopathy can typically be made through appropriate history and physical exam. Sungazing, eclipse viewing, occupational hazards (such as welding without a welding helmet or welding goggles) exposure to lasers or laser pointers, or recent cataract extraction or other ophthalmologic operative procedures all have been associated with retinopathy. Patients typically present with central blurred vision or dark scotoma in one or both eyes. Patients may also endorse metamorphopsias, micropsia, or headaches. Initial visual acuity varies and typically is between 20/20 to 20/100 however could be worse depending on extent of exposure.
Exam and imaging findings tend to be bilateral and symmetric. OCT typically shows focal disruption at the level of the sub-foveal RPE and outer retinal bands with normal inner retinal layers. The isolation of changes to the outer retina is almost universally present in cases of solar retinopathy. Punctate RPE window defects can be seen on FA. OCT can be used to monitor disease and typically shows resolution to outer retinal changes as symptoms resolve.
There is no proven treatment for solar retinopathy, but patients typically have spontaneous resolution within 1 to 6 months after injury. Even in patients with significant vision loss at presentation, most patients ultimately have visual acuity between 20/20 to 20/40. Metamorphopsias or central/paracentral scotomas may remain permanent.
If you are looking to schedule your first consultation, please contact us today by clicking HERE and find the location that is nearest you!
References:
-
Yannuzi LA, Fisher YL, KruegerA, et al. Solar Retinopathy: A photobiological and geophysical analysis. Tr. Am. Ophth Soc. 1987; 85:120-158. - American Academy of Ophthalmology. “Solar Retinopathy.” Section 12: Retina and Vitreous. Singapore, 2013-2014. 332-334.
- Youseff PN, Sheibani N, Albert DM. Retinal light toxicity. Eye (Lond). 2011; 25(1):1-14.
- Atmaca LS1, Idil A, Can D. Early and late visual prognosis in solar retinopathy. Graefes Arch Clin Exp Ophthalmol. 1995; 233(12):801-4.
- Rothkoff L, Kushelevsky A, Blumenthal M. Solar retinopathy: visual prognosis in 20 cases. Isr J Med Sci. 1978; 14(2):238-43.