Serpiginous Choroidopathy – August, 2024

History:
A 65-year-old female presented with blurry vision in the left eye (OS) that had progressively worsened over years.
Exam:
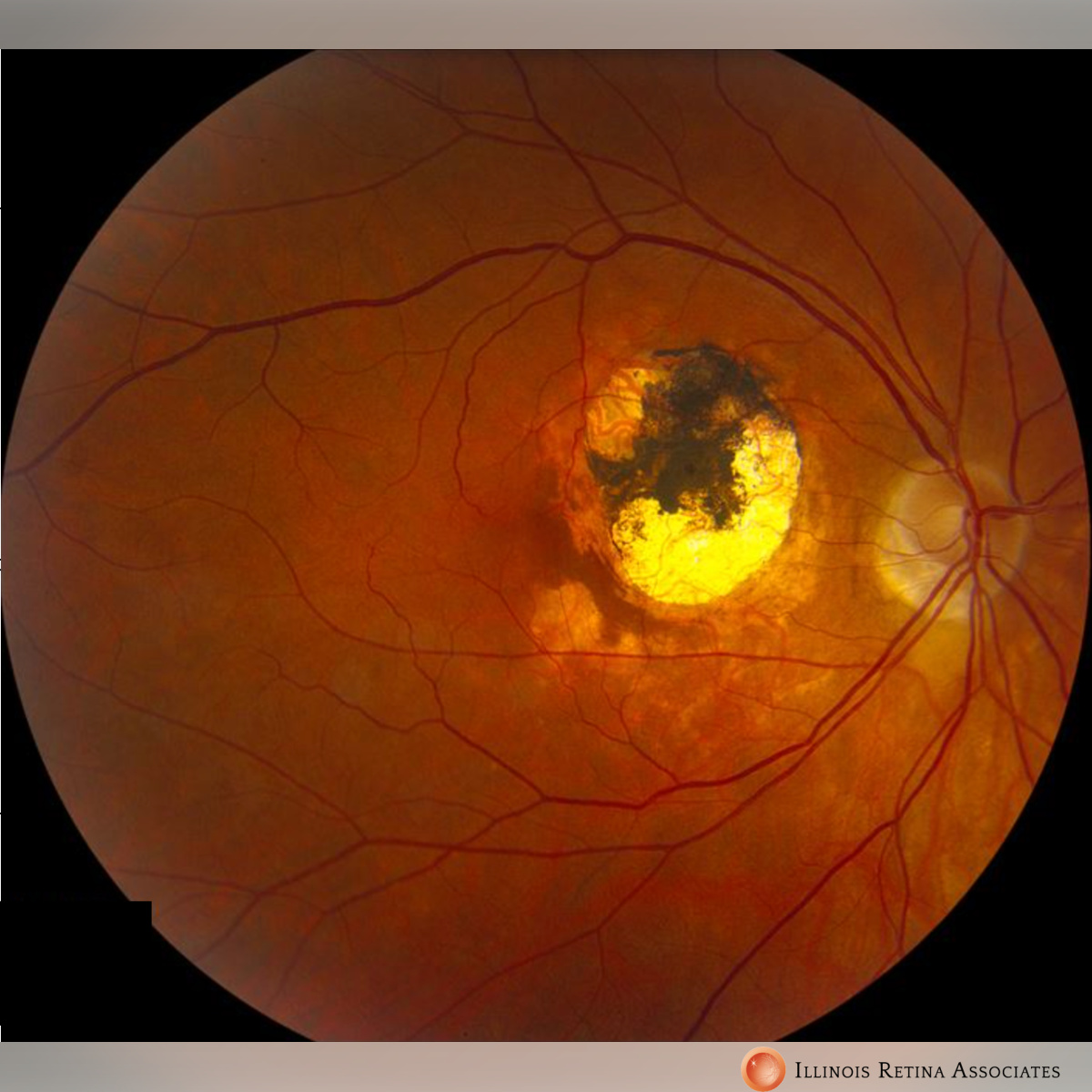
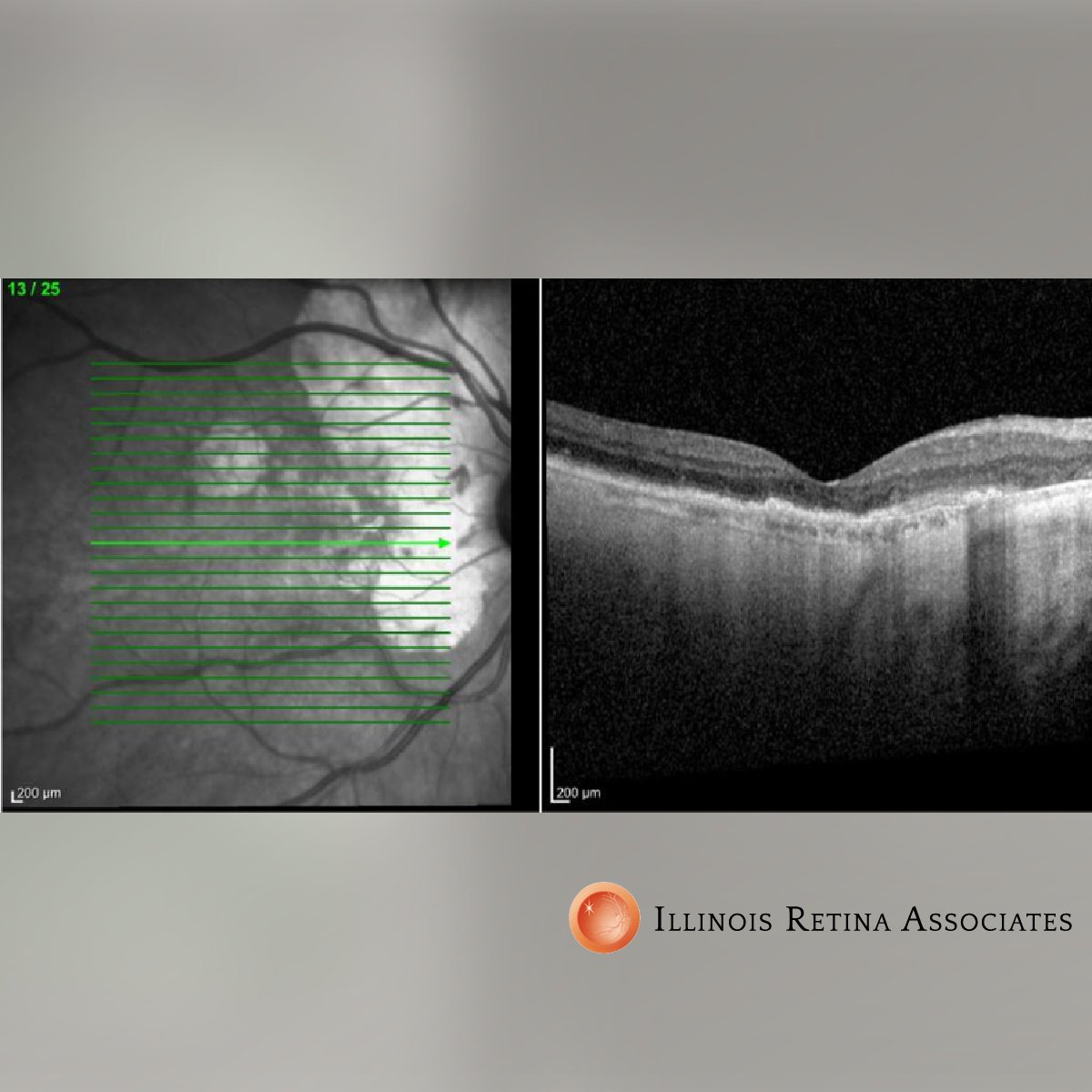
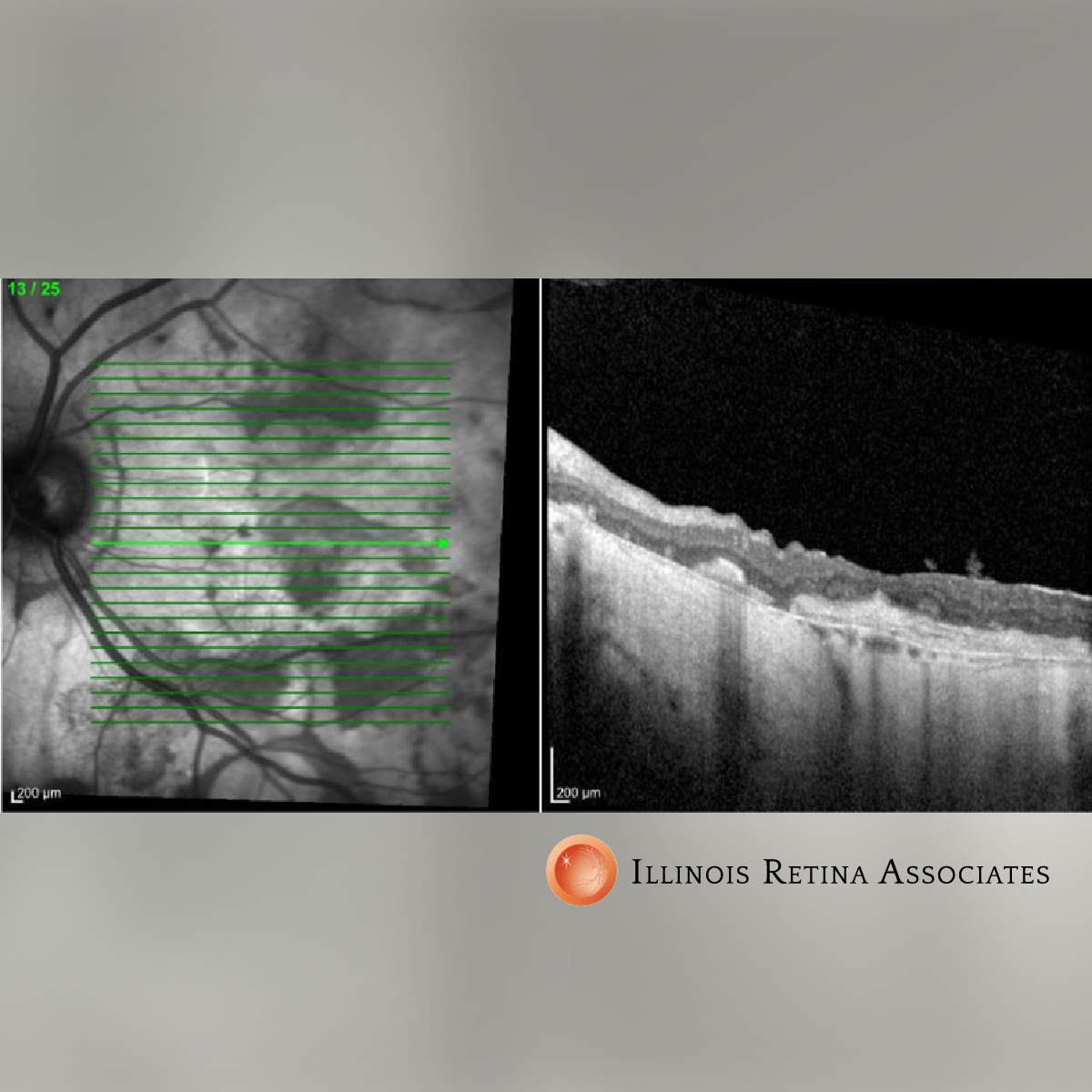
Visual acuity (VA) was 20/40 in the right eye (OD) and count fingers (CF) OS, and intraocular pressure (IOP) was normal in both eyes (OU). Anterior segment exam revealed 2+ nuclear sclerosis OU. Dilated fundus exam revealed no vitritis. There was large peripapillary atrophy OD. There was an even larger area of well-circumscribed atrophy with areas of hyperpigmentation extending from the optic nerve to the macula OS (Figures 1 and 2). OCT demonstrated patchy outer retinal atrophy OD and diffuse outer retinal atrophy with subretinal fibrosis OS (Figures 3 and 4).

The patient reported having received multiple treatment of anti-VEGF for active CNV in the past.
Differential Diagnosis:
• Serpiginous Choroidopathy
• TB-associated Serpiginous-like Choroidopathy
• Multifocal Chorioretinitis
• Acute Posterior Multifocal Placoid Pigment Epitheliopathy
• Toxoplasmosis
Discussion:
Serpiginous Choroidopathy
Serpiginous choroidopathy is a rare auto-immune condition with poorly understood pathophysiology, which accounts for less than 5% of posterior uveitis cases. It affects middle-aged adults--men more than women. It is a bilateral condition, usually affecting one eye more than the other.
Patients typically present with painless unilateral scotoma. Diagnosis is clinical with yellow subretinal infiltrates spreading centrifugally from optic nerve head in a snake-like (serpiginous) manner. It is imperative to rule out TB as a cause, as the appearance is similar. The mainstay of treatment of active disease are steroids and immunosuppressants.
Prognosis can be poor, especially with large lesions affecting the macula. Up to 25% of eyes have a final visual acuity of less than 20/200. Choroidopathy typically has many recurrences with variable intervals which could range from months to years. CNV can affect up to 35% of patients and accounts for the most common complication. Other complications include subretinal fibrosis, macular edema, vein occlusion, and serous retinal detachment.
If you are looking to schedule your first consultation, please contact us today by clicking HERE and find the location that is nearest you!
References:
-
Nazari Khanamiri H, Rao NA. Serpiginous choroiditis and infectious multifocal serpiginoid choroiditis. Surv Ophthalmol. 2013 May-Jun;58(3):203-32. - Akpek EK, Jabs DA, Tessler HH, Joondeph BC, Foster CS. Sucessful treatment of serpiginous choroiditis with alkylating agents. Ophthalmology. 2002; 109(8): 1506-13.
- Ciulla TA, Gragoudas ES. Serpiginous choroiditis. Int Ophthalmol Clin. 1996; 36:135-43.