North Carolina Macular Dystrophy – July, 2024

History:
A 42-year-old male presented for a second opinion after being diagnosed with bilateral ocular toxoplasmosis. He had no visual symptoms and reported trauma to the eyes with a stick when he was 10 years old. There was no family history of retinal disease.
Exam:
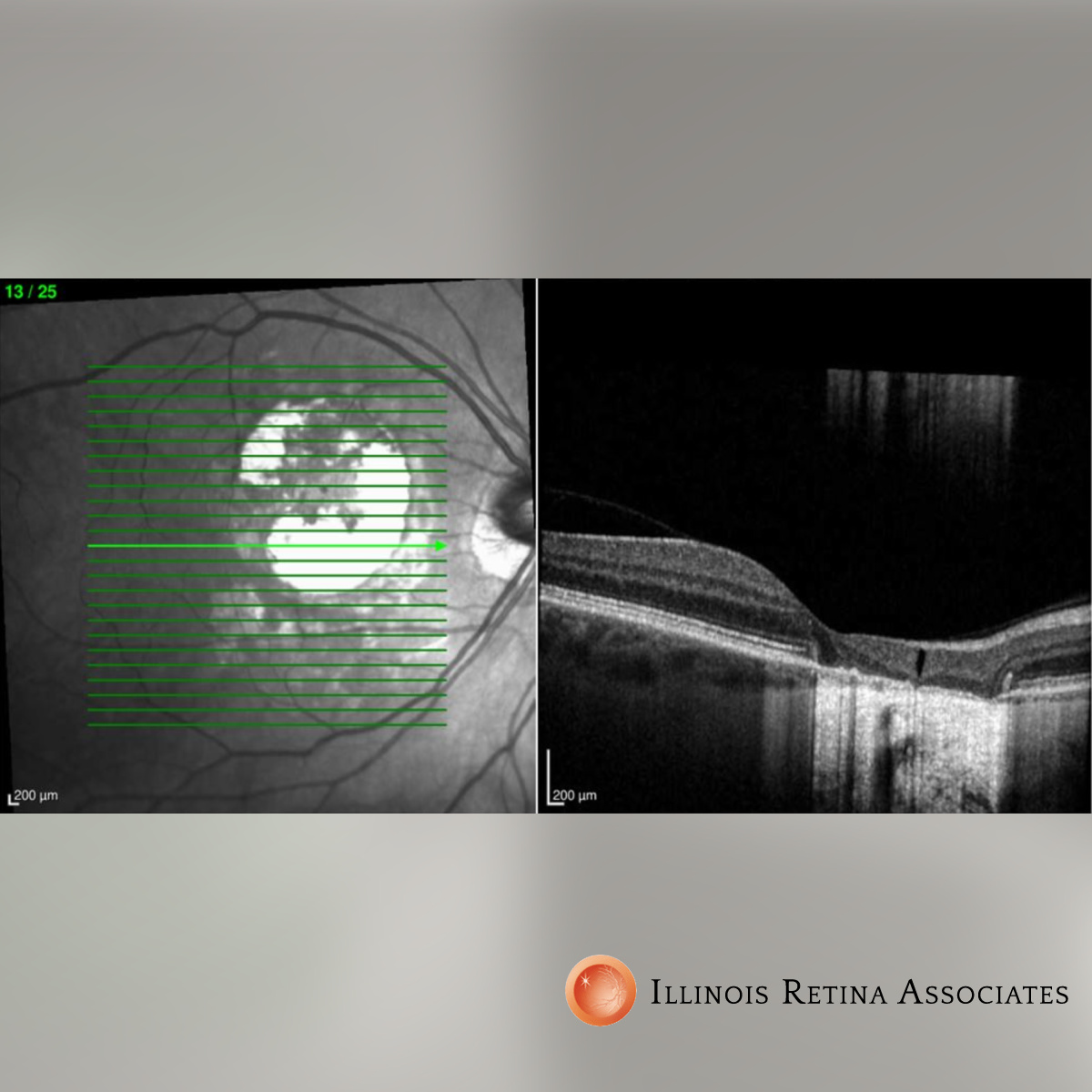
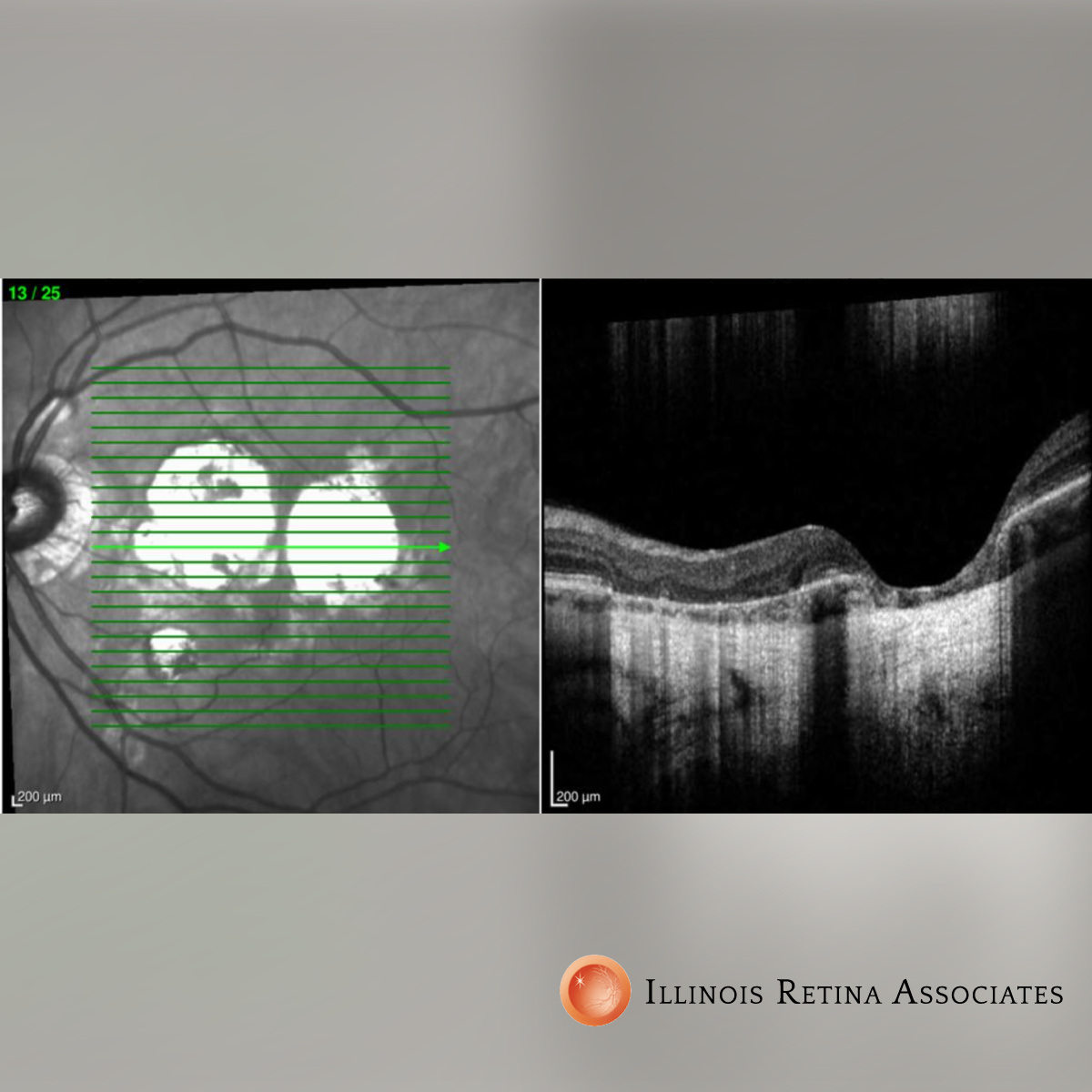
Visual acuity was 20/25 and 20/20, and intraocular pressures were normal OU. Color vision was normal. Anterior segment exam was unremarkable. Dilated fundus exam revealed a large central area of RPE atrophy in the right eye and multiple patches of RPE atrophy in the left eye (Fig 1 and 2). Retinal periphery was normal. OCT demonstrated areas of atrophy of the RPE and choriocapillaris that bowed back into the sclera which corresponded to the lesions seen on exam (Fig 3 and 4). Fluorescein angiogram revealed no leakage. A clinical diagnosis of North Carolina Macular Dystrophy was made based on the above findings.


Differential Diagnosis:
• Congenital toxoplasmosis
• Best vitelliform macular dystrophy
• Age-related macular degeneration
• Torpedo maculopathy
• Cone dystrophy
Discussion:
North Carolina Macular Dystrophy
North Carolina Macular Dystrophy (NCMD) is an inherited autosomal dominant retinal dystrophy which was first discovered in a large family in North Carolina. 30% of patients are asymptomatic while a third have mild visual symptoms, and another third suffer moderate central visual impairment. Severe visual impairment can occur in a few patients due to choroidal neovascular membranes (CNVM).
Diagnosis is primarily clinical and there is variable expressivity in phenotype. Lesions are typically bilaterally symmetrical and can vary from central small or intermediate drusen (grade 1), to confluent drusen and central vitelliform lesions (grade 2), to large central coloboma-like defects (grade 3) which often have surrounding subretinal fibrosis from CNVM.
Visual acuity is surprisingly good for the OCT findings and visual acuity stabilizes during the patient’s lifetime unless a central CNVM forms. There is no treatment, however patients are periodically monitored for CNVM which are treated with anti-VEGF injections. Prognosis is good for maintaining good functional vision throughout life, however CNVM should be treated when present.
If you are looking to schedule your first consultation, please contact us today by clicking HERE and find the location that is nearest you!
References:
-
Small KW, DeLuca AP, Whitmore SS, Rosenberg T, Silva-Garcia R, Udar N, Puech B, Garcia CA, Rice TA, Fishman GA, Héon E, Folk JC, Streb LM, Haas CM, Wiley LA, Scheetz TE, Fingert JH, Mullins RF, Tucker BA, Stone EM. North Carolina Macular Dystrophy Is Caused by Dysregulation of the Retinal Transcription Factor PRDM13. Ophthalmology 123:9-18, 2016 - Green DJ, Lenassi E, Manning CS, McGaughey D, Sharma V, Black GC, Ellingford JM, Sergouniotis PI. North Carolina Macular Dystrophy: Phenotypic Variability and Computational Analysis of Disease-Associated Noncoding Variants. Invest Ophthalmol Vis Sci. 2021 Jun 1;62(7):16. doi: 10.1167/iovs.62.7.16.
- Bakall B, Bryan JS 3rd, Stone EM, Small KW. Choroidal Neovascularization in North Carolina Macular Dystrophy Responsive to Anti-Vascular Endothelial Growth Factory Therapy. Retin Cases Brief Rep. 2021 Sep 1;15(5):509-513. doi: 10.1097/ICB.0000000000000838. PMID: 30383557.