High Altitude Retinopathy – February 2020

History
A 32 year old female presents with sudden vision loss in the left eye. She notes it as a grey thumb print in her left eye and noticed it while she was washing dishes. She denies any physical exertion surrounding the vision loss, but she notes that the day before she was skiing difficult trails at an elevation of 13,000 feet and did not have any water because her water bottle had frozen.
Exam:
Her vision in the right eye was 20/20 with correction, but 20/400 in the left eye with no improvement with pinhole. She had no APD, and IOP was 13 and 11. Her confrontational fields were full as was her motility. Her anterior segment exam was normal, with no inflammation and no cataract.
Examination of the posterior segment is demonstrated in the following photos:
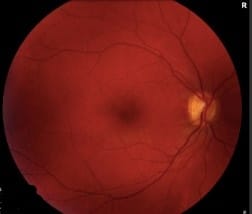

Fundus photographs of the posterior pole: The right eye is normal. The left eye demonstrates slight venous tortuosity, a large preretinal/sub-ILM hemorrhage, a superior subretinal hemorrhage, and a small flame hemorrhage along the inferotemporal arcade.
Further imaging was obained:
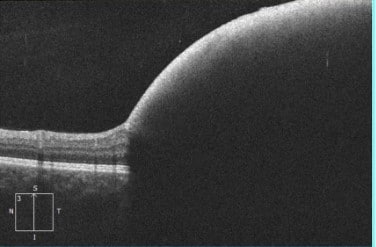
OCT of the left eye demonstrating a large sub-ILM hemorrhage with blockage of reflection. The right eye was normal.
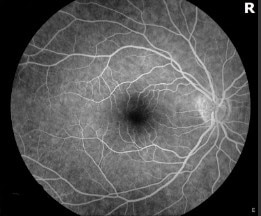
Florescein Angiogram: The right eye is normal. The left eye demonstrates blocking from the hemorrhages seen on exam. There was no delayed filling of the veins. There was no evidence of retinal macroaneurysm.

Differential Diagnosis:
- Valsalva retinopathy
- Macroaneurysm
- High Altitude Retinopathy
- Central retinal vein occlusion
- Tersons syndrome
The decision was made to observe the patient closely. She was also referred to her PCP for systemic workup of blood pressure and hypercoagulable states associated with CRVO. This testing was all normal. When she returned 1 week later, her preretinal/sub-ILM hemorrhage had mildly worsened:

Discussion:
High Altitude Retinopathy
Given the patients young age, healthy lifestyle, and exposure to high altitude with relative dehydration, the most likely diagnosis is high altitude retinopathy. She is unlikely to have a microaneurysm given her normal blood pressure. Also, she was not straining at all the time surrounding the vision loss, making Valsalva retinopathy less likely. Though there may be some very slight venous tortuosity, there was no delayed filling on FA.
High altitude retinopathy (HAR) is well described in the literature in mountaineers. Typically, these cases occur in patients who ascend to heights above 12,000 ft1. HAR is marked by retinal, sub-ILM, preretinal and even vitreous hemorrhages as well as Roth spots and disc edema. These findings can persist for weeks after return to normal altitude but resolve with time2. Barthelemes et al reported a study where 31 patients had fundus photography along their ascent and descent of Mt Mustagh Ata (24,751 ft). Along the way up, we noted minimal hemorrhages. However, hemorrhages increased during the descent. 79% of patients demonstrated retinal hemorrhages in this study. They also noted the hemorrhages were correlated with decreased oxygen saturation during the climb. Thus, they posit that these hemorrhages are related to hypoxic damage to the vascular endothelium, increasing permeability. In addition, higher hematocrit also correlated with more hemorrhages, possibly secondary to shear stress on the already damaged vascular endothelial cells3. It seems likely that given our patient’s activity (very difficult skiing) and dehydration, she likely had a combination of low oxygen saturation and higher than usual hematorcrit, possibly increasing her risk of high altitude retinopathy at the relatively low height of 13,000 ft.
If you are looking to schedule your first consultation, please contact us today by clicking HERE and find the location that is nearest you!
References:
- Shults WT, Swan KC. High altitude retinopathy in mountain climbers. Arch Ophthalmol. 1975;93(6):404–408. doi:10.1001/archopht.1975.01010020418003
- MAcLARENRE, IKRAM K, TALKSFluorescein angiography in altitude retinopathy. British Journal of Ophthalmology 2000;84:337.
- Barthelmes D, Bosch MM, Merz TM, et al. Delayed appearance of high altitude retinal hemorrhages. PLoS One. 2011;6(2):e11532. Published 2011 Feb 17. doi:10.1371/journal.pone.0011532